Latest in Health & Science News
Get up-to-date health & science news from our reporters
Prescription drugs lack country-of-origin labels. Senators object.
The FDA allows drug manufacturers to keep confidential information about where prescription drugs and their ingredients are produced.
read more
The Doomsday Clock moves closer to apocalypse than ever
The Bulletin of Atomic Scientists set the Doomsday clock four seconds closer to midnight than last year due to insufficient progress in addressing the global existential threats.
read more
Lawmakers question health insurance CEOs on rising costs
The hearing hosted CEOs from UnitedHealth Group, CVS Health, Elevance Health, Cigna Group and Ascendium.
read more
Lawmakers struggle to find consensus on health care reforms
While House Republicans and Democrats did not agree on paths to health care cost reforms, they found common ground on breaking up market consolidation.
read more
Senate Republicans call for a safety review of chemical abortion drugs
Lawmakers clashed Wednesday over the mail delivery of abortion drugs and the safety of one of them, mifepristone.
read moreListen: Diaspora-led medical organizations are rebuilding care in Palestine and Sudan
WASHINGTON — Diaspora-led medical organizations operate in conflict zones with local knowledge, long-term commitment and trusted networks. Their work spans direct care, training, local funding, and infrastructure support — offering an alternative approach to international aid models.
In this episode, we look at the Palestinian American Medical Association and the Sudanese American Medical Association, and the impact their different approaches are having on the ground.
Supreme Court hears case on faith-based pregnancy center’s free speech subpoena challenge
WASHINGTON — The Supreme Court heard a case Tuesday on whether First Choice Women’s Resource Center, a New Jersey faith-based pregnancy center, can challenge a state subpoena in federal court before it is enforced.
New Jersey issued a subpoena seeking 28 categories of documents about the centers’ practices, including a list of donors, as part of an investigation into whether First Choice was misleading potential clients about their services.
First Choice sued New Jersey in December 2023, alleging that the subpoena violated its First Amendment rights and created a chilling effect on donors.
The subpoena at the heart of the dispute is non-self-executing, meaning that a court order is required for its enforcement. First Choice argues that the subpoena’s existence, even before it’s executed, is not without penalties.
“It says that if you fail to obey the subpoena again — not a later court order — if you fail to obey the subpoena, you could be subject to contempt, you could lose your business license,” Erin Hawley, the attorney for First Choice, said. “Those are the death knell for nonprofits like First Choice.”
While the case is working its way through state court, First Choice went to federal court with a civil rights claim, but was told the case was “unripe”. A central legal question in front of the Supreme Court on Tuesday was whether the case was “ripe” enough to be heard in federal court.
First Choice argued that the chilling effect of the subpoena was a “burden” on the center, which made the case “ripe” enough. Justice Ketanji Brown Jackson questioned whether the subpoena had actually caused real harm before its enforcement.
“Even if we agree that your constitutional rights are arguably burdened, is it really occurring at the moment of receipt of the subpoena?” Jackson said.
New Jersey argued that First Choice’s claims are “tethered to a future downstream state court order” and not to the subpoena itself. Sundeep Iyer, the chief counsel to the New Jersey Attorney General, said that there was no evidence of actually being chilled by the subpoena over the last two years of litigation.
Chief Justice John Roberts questioned how such evidence could be gathered in the first place.
“Well, how do you get that evidence? Somebody comes in and says, ‘I’m chilled, I don’t want to reveal my name, address, phone number, et cetera, and here is my affidavit,’” Roberts said. “That’s not going to work, is it?”
Several nonprofits across the country have filed amicus briefs for First Choice, arguing that the case could majorly impact free association and speech in organizations nationwide.
Grayson Clary, staff attorney at the Reporters Committee for Freedom of the Press, said that several media outlets have received similar subpoenas, citing the Federal Trade Commission’s recent demands for internal records from watchdog nonprofit Media Matters.
“It makes sources less willing to talk to you, if they worry that speaking to you is going to get them dragged into some kind of investigation like this, and so the consequences can be really chilling,” Clary said.
However, Clary felt the oral argument was encouraging, noting how justices from both sides of the ideological spectrum were more skeptical of New Jersey’s claims.
“It’s always hard to read the tea leaves, but it sounded like a majority of the justices shared that attitude, and we certainly hope that’s the direction they’ll go in the ruling,” Clary said.
In an amicus brief, the ACLU argued that such First Amendment cases are important so that state investigatory tools aren’t used for retaliation.
“To ensure that these investigatory tools are not abused to retaliate against the ideological opponents of those in office, federal courts must promptly review claims that law enforcement subpoenas violate the First Amendment.”
Warnings over US dependence on foreign generic drug supply threaten quality and access to medications
WASHINGTON — Pharmaceutical executives and lawmakers warned that the United States’ reliance on foreign nations for key pharmaceutical components is disrupting the quality and access American patients have to generic medications at a Senate Special Committee on Aging hearing on Wednesday.
“We’ve seen the results of that dependence,” said Committee Chairman Sen. Rick Scott (R-Fla.). “Contaminated drugs, dangerous recalls and shortages that force doctors and patients to ration care.”
In particular, experts cautioned against relying on foreign nations for active pharmaceutical ingredients (APIs), the most important component of a drug that provides the clinical effects of a medication.
Over 80% of APIs used in U.S. prescription drugs don’t have a domestic source, according to a study from Washington University in St. Louis. China primarily dominates the initial stages of the pharmaceutical supply chain: taking the starting compounds and synthesizing them into APIs.
American manufacturers then integrate APIs into the final dosage form to sell to wholesalers, who will distribute the product to pharmacies and hospitals. The structure of the supply chain forces American manufacturers to be dependent on other nations for the building blocks of the medications sold in the U.S.
But running a pharmaceutical plant is significantly cheaper in countries including China and India compared to the U.S., in part due to subsidies foreign governments provide to incentivize companies for their pharmaceutical exports, said Tom Neely, Chairman of Oxford Pharmaceuticals, a generic drug manufacturer in the U.S.
“Every tablet that leaves our factory is undercut by foreign government-subsidized competitors who treat medicine as a strategic export,” Neely said in written testimony. “The current U.S. trade model has distorted and manipulated the market, directly harming U.S. manufacturers like us and ultimately the well-being of American citizens.”
Experts also raised concerns about the drug safety standards of foreign manufacturing plants compared to those in U.S. facilities. Manufacturing plants in the U.S. operate under strict FDA guidelines, including continuous, surprise inspections, Neely said, while many foreign facilities go long periods without inspections and receive advance notice of the oversight.
A ProPublica investigation published in June revealed that the FDA allowed over 20 foreign factories to continue exporting drugs to the U.S. despite previously banning the plants because of manufacturing violations, raising questions about health risks from foreign-sourced drugs.
In October, the FDA identified significant safety violations at a generic manufacturing facility in India, including the presence of animals in API drums and contaminated storage environments.
“Is it too much to ask that plants don’t have flying birds and skittering lizards?” Sen. Scott said, referring to the FDA’s findings.
Patrick Cashman, the president of USAntibiotics, called on the federal government to create more opportunities for domestic manufacturers to be more competitive, including demanding greater transparency in pharmaceutical supply chains and government assurance of demand despite low-cost foreign production.
Domestic pharmaceutical manufacturing holds the same importance as semiconductor and defense manufacturing, Cashman said in written testimony.
“We are not asking for subsidies or handouts,” Cashman said at the hearing. “We are asking that when the government buys antibiotics, it prioritizes genuine, American manufacturing.”
Senate examines soaring health care costs, new policy paths ahead of tax credit expiration
WASHINGTON – The Senate Finance Committee debated proposals to address rising health care costs and alternatives to the Affordable Care Act (ACA) subsidies set to expire at the end of this year during a hearing on Wednesday.
The hearing comes in the aftermath of a prolonged government shutdown in which health care funding and tax-credit extensions emerged as central flashpoints. Roughly 93% of those who purchase insurance through the ACA marketplace received subsidies from the government in 2025.
If Congress does not pass legislation to extend the credits into 2026—a key demand of Democrats during the government shutdown—premium payments will more than double. Lawmakers on both sides of the aisle agreed on the broader health care affordability crisis plaguing Americans but differed on the appropriate path forward.
“Our health care system is broken,” Committee Chairman Mike Crapo (R-Idaho) said.
“Obamacare failed to make health care more affordable.”
Sen. Bill Cassidy (R-La.), chairman of the Senate Health, Education, Labor and Pensions Committee, proposed an alternative to ACA credits that closely aligns with President Donald Trump’s approach.
Under Cassidy’s proposal, eligible Americans would receive a pre-funded flexible spending account when opting into a bronze-level plan, which has the lowest premiums and highest out-of-pocket costs.
“Under the status quo my colleagues are pushing, 20% is going to the insurance company for overhead and for profit,” Cassidy said. “What we are proposing is that 100% goes to a patient-driven account which you can use for a physician or dentist or drugs.”
Brian Blase, president of the Paragon Health Institute, said in written testimony that pandemic-era subsidies have fueled the “ACA’s premium spiral.” He proposed several affordability solutions, including tax-favored accounts that give consumers more control over their health care spending.
“Extending temporary emergency subsidies would deepen our broken system instead of fixing it,” Blase said.
Senate Democrats dismissed this approach and raised doubts about Republicans passing new and effective legislation by the end of the year.
According to Ranking Member Ron Wyden (D-Ore.), there is “no way” for Congress to build a proposal that will help those affected by rising ACA premiums before January. Wyden said spending accounts can be a “useful tool for very wealthy people” but not a “comprehensive health insurance opportunity” for all.
Wyden introduced Bartley Armitage, a retiree from Oregon, as a witness before the committee. Armitage’s testimony focused on the personal toll of rising insurance costs, especially the monthly premium hike from $443 to $2,224 in his family’s ACA plan next year.
“Nobody wants to pay that kind of bill for one month, and most can’t afford it,” Armitage said. “A bill like that is like having to pay for two houses.”
“I urge you to take action that keeps our health costs affordable before we’re hit with a massive bill this January,” he added.
Senate Majority Leader John Thune (R-S.D.) promised Democrats a vote on ACA subsidies by the end of the second week of December, a move that led some Democrats to break with the party and vote in favor of the funding bill to reopen the government last week.
In addition to passing the Senate, a Democrat-sponsored bill must pass the House and secure Trump’s signature before ACA enrollees make their first payment for next year. But, the president urged Congress not to “waste” time on negotiating the subsidies in a Truth Social post on Tuesday, stating that he would only support a plan that sends money “directly back to the people.”
Despite Trump’s comments, lawmakers present at Wednesday’s hearings supported continued bipartisan efforts.
“I think everybody on this committee is all in for trying to work together to find those bipartisan solutions to make health care affordable,” Crapo said.
RFK Jr. touts ‘Make America Healthy Again’ agenda to divided audience at GW University
WASHINGTON — Health Secretary Robert F. Kennedy Jr. pitched his Make America Healthy Again (MAHA) movement as a disruptive force in health policy at a “fireside chat” hosted by Turning Point USA-Foggy Bottom on Monday evening.
Organizers intended the event at George Washington University to be an exercise of free speech and inquiry, in honor of late right-wing activist Charlie Kirk. Kennedy faced a polarized audience as he reiterated his mission to end chronic diseases in the U.S.
“(My goal is) to end the chronic disease crisis and make America the healthiest nation in the world, like it was when I was a kid,” Kennedy said.
Nearly 100 students protested outside the venue, criticizing Kennedy’s frequent vaccine misinformation and his comments on people with autism. GWU’s Disabled Students Collective also circulated a petition urging university administrators to prevent Kennedy from speaking on campus.
RJ Doroshewitz, president of GWU’s chapter of Democracy Matters, said Kennedy has spread “baseless conspiracy theories” and has harmed marginalized communities at the university, including transgeneder students and students with autism.
“We believe in truth. We believe in the rule of law. We believe in science,” Doroshewitz said. “RFK — I wish he did, but he does not reflect any of those values.”
Inside the event, the crowd mostly cheered for Kennedy as he doubled down on some of his more controversial positions.
Kennedy claimed antidepressant SSRI drugs are a possible cause of mass shootings, insisted that the Trump administration had not cut funds for clinical trials, reframed pandemic-era public health measures as constitutional violations and praised recent HHS efforts to initiate studies on the link between vaccines and autism.
There is no evidence that SSRIs cause people to commit mass shootings, the National Institutes of Health terminated grants for 383 clinical trials between Feb. 28 and Aug. 15, federal courts have upheld states’ authority to enact public health laws and rejected claims that refusal to mask was protected speech and multiple peer-reviewed studies have rebuked Kennedy’s claim that vaccines cause autism.
The event was the first hosted by the brand-new Foggy Bottom chapter of TPUSA. Chapter President Ryan Van Slingerland and GWU College Republicans Vice Chairman Paul Lieb co-moderated the discussion.
Lieb told Medill News Service the chapter chose to host Kennedy because of his influence within the Trump administration, and added that Kennedy has made “a lot of effective changes.”
“It’s hard to go up there, especially when you are the secretary of one of the most influential departments in the entire nation and then trying to defend every little thing, especially to college students,” Lieb said.
As the Q&A portion began, dozens of audience members rushed to line up to ask Kennedy a question, pressing him on his public health qualifications, mass HHS firings, food labeling and the opioid epidemic. One student asked Kennedy about his anti-vaccine claims, to which Kennedy replied: “I believe what I’ve always believed.”
Zach Novick, who attended the event, said the questions, and the protest, largely focused on concerns about national issues and reflected deep societal polarization, but added that he appreciated the organizers’ goal of civil discussion.
“(Kennedy) is such an interesting figure within current politics. I can’t really think of anyone else that I know who’s like him,” Novick said. “I think it’s good that he’s out here trying to at least communicate what he’s feeling.”
Novick said he was particularly interested in Kennedy’s claim that federal agencies had long been influenced by special interests such as the pharmaceutical industry.
Throughout the event, Kennedy framed the MAHA movement as a bipartisan agenda blocked by partisan optics, not by substance. He claimed Democratic governors privately agree with him on food dye bans, SNAP waivers and whole-food school lunches, but refuse to adopt the MAHA label.
Kennedy also argued the rise of chronic diseases is an issue that uniquely impacts younger generations. He blamed his own generation for failing young people, but said that his movement would give them the information to address the environmental causes of chronic disease.
Watch the Video Report Here:
WATCH: Public Health Advocates Host Historic D.C. Rally
WASHINGTON — Hundreds of public health advocates gathered on the National Mall on Wednesday to challenge key public health issues, including Medicaid cuts, vaccinations and reproductive rights.
The rally marked the end of the American Public Health Association’s annual D.C. meeting, with attendees ranging from physicians to workers from the Centers for Disease Control and Prevention.
Several rally speakers called for Health and Human Services Secretary Robert F. Kennedy Jr. to be fired, criticizing the Make America Healthy Again movement Jr. leads.
“One of Jr.’s first acts was to put out the MAHA report on children’s health,” said Bob Morris, the Founder of the Science Accountability Institute. Well, if he truly cared about children’s health, he’d worry more about bullets in their heads than the coloring in their skittles.”
Watch the video report here:
Soybean oil’s time to shine
WASHINGTON — For the first time in seven years, China did not purchase a single bushel of soybeans from the United States this summer as the two countries remain in economic conflict. This comes just one year after China purchased 27 million metric tons of American soybeans, amounting to $12.6 billion.
American farmers have long relied on China’s massive demand for soybean meal, a high-protein animal feed. Now, as China turns to Brazil and Argentina to meet its soybean needs, U.S. farmers are left scrambling to sell their crops.
“Let’s be clear, this is a man-made disaster caused by Donald Trump and his administration,” soybean farmer John Bartman said at a press call hosted by the Democratic National Committee in October. “Why? Because there’s nearly 1 billion bushels of soybeans that don’t have a home right now.”
The scale of the disaster
U.S. farmers will lose roughly $100 per acre this year, according to the University of Illinois Urbana-Champaign. For Adam Phelon, who planted over 1,000 acres of soybeans on his family farm in Melvern, Kan., that could mean a $100,000 loss in gross income.
“It’s been 40 years of market development that’s taken place to get it to where we are, and so having that just eroded away, we can’t just replace that overnight,” Phelon said in an interview. “We’re going to see lasting effects for years to come.”
Grain market economist Ed Usset said he’s concerned about the long-term implications of losing China’s business, specifically if China learns it no longer needs the United States to fulfill its soybean needs.
Minnesota Gov. Tim Walz expressed similar sentiments, calling on Trump to end the “ridiculous trade war” and recognize the long-lasting damage China’s boycott will have on rural America.
“The thing we need to keep in mind is it took decades to establish these markets,” Walz said during the press call. “China didn’t just sign one-year contracts with Argentina. They signed some of them up to a decade-long, and it’s going to take us years to get these markets back.”
In September, Argentina temporarily suspended its 26% soybean export tax in an attempt to boost sales. China then purchased 7 million metric tons of Argentine soybeans, to the dismay of American farmers. Phelon was further angered to see President Trump finalize a $20 billion bailout to stimulate Argentina’s economy, calling the move “a kick in the pants to farmers.”
Soybean oil as a solution
As the United States searches for other export markets for American soybeans, the expanding biofuels market offers a promising opportunity to drive domestic demand — specifically, for soybean oil.
Historically, soybean meal has contributed much more to driving the value of a bushel, according to Scott Irwin, an agricultural marketing professor at the University of Illinois Urbana-Champaign.
“A rule of thumb was that around two-thirds of the value of a bushel of soybeans could be traced to soybean meal,” Irwin said. “That has dropped to 50–55% with the boom in biodiesel and renewable diesel production, particularly the latter.”
Soybean oil can be processed into renewable diesel, a sustainable fuel made from plants or animal fats that is chemically identical to petroleum, but much better for the environment because, like all plants, soybeans absorb carbon dioxide as they grow rather than raising greenhouse gas emissions.
In June, the Environmental Protection Agency proposed raising minimum volume mandates for the use of different biofuels under the Renewable Fuel Standard (RFS) for 2026 and 2027. The proposal would increase the amount of renewable fuel required to be blended into U.S. transportation fuel, like the diesel fuel truckers use to fill their tanks.
If the EPA proposal becomes a final regulation, it will mandate the highest renewable fuel blending standards in American history. The development would heavily benefit soybean farmers by driving the demand for soybean oil to fulfill the EPA’s regulations, Irwin said.
Greenhouse gases produced by advanced biofuels stay in the atmosphere for half as long as gases generated from petroleum, Irwin said.
“On that front, surprisingly, the Trump administration is encouraging something that’s positive from a greenhouse gas climate perspective,” Irwin said.
Renewable diesel is considered a “drop-in” substitute for petroleum diesel, Scott Gerlt, the Chief Economist of the American Soybean Association, told Planet Forward in an interview. From an engineering perspective, that means renewable diesel can be used as a replacement for petroleum diesel without worrying about changing infrastructure or blending levels.
Soybean oil’s potential doesn’t stop at the fuel pump. Researchers Eric Cochran and Chris Williams from Iowa State University are taking soybean oil to the roads: Their soybean-based asphalt polymer can replace petroleum additives, making pavement both longer lasting and more sustainable.
The traditional polymer additive used in asphalt is SPS, a purely petroleum-based polymer that is rarely manufactured domestically nowadays. A key component of SPS called butadiene can also be hazardous to handle, Cochran said. Soybean oil, on the other hand, reduces reliance on petroleum products while supporting the domestic soybean market.
“Making your pavements last longer means less raw material, less energy, less fuel needed for all that construction, and then the materials that are going into the pavements become increasingly U.S. agriculturally sourced,” Cochran said.
Cochran said the product is currently being manufactured across the United States and sold to county engineers, contractors, asphalt terminals, and oil refineries. Over the next year, homeowners can look out for do-it-yourself products for roofing and driveway maintenance.
In the meantime, the Trump administration is expected to announce a relief plan of at least $10 billion for farmers hurt by tariffs. Still, farmers have said the temporary fix doesn’t provide what they actually want, and what soybean oil might give them a chance to do: to compete fairly in the global marketplace.
“This is our livelihood. We need to make sure that we have a place to go with our soybeans,” Phelon said. “That’s the number one goal. We want to feed and fuel the world, and without trade around the world, we’re not able to do that.”
Published in conjunction with ![]()
Senate Republicans, conservative think tanks criticize Affordable Care Act
WASHINGTON — Republican senators and witnesses criticized the affordability of the ACA on Thursday, claiming the health care plan drives up costs and stifles competition. In a contentious hearing with the Homeland Security & Governmental Affairs Subcommittee on Investigations, witnesses across the health care industry condemned the fiscal impacts of the ACA, also called Obamacare.
Senator Ron Johnson (R-Wis.) said that the ACA harmed the health care market.
“The third-party data system has led to greater consolidation within all sectors of health care industry, medically reducing competition and driving up costs,” Johnson said.
He also criticized the fiscal spending of Medicaid, claiming that the Affordable Care Act cleared the way for high government spending for health care coverage.
“Instead of acknowledging all the damage done by the default design of Obamacare and working in good faith with Republicans to repair it, Democrats simply want to spend hundreds of billions of dollars more in their attempt to continue to hide this failure,” Johnson added.
Joel White, President of Council for Affordable Health Coverage, said that the ACA’s consolidation of health care coverage comes at the expense of quality care.
The Council for Affordable Health Coverage advocates for increased competition in the health care market, seeking more options for consumers.
“We are subsidizing inferior coverage through incentives created…Why is this happening? A big reason is that Obamacare drove consolidation and triggered an arms race to consolidate in insurance markets and hospital markets, and that is driving up costs in the market and leaving consumers with fewer choices,” he said.
According to Tarren Bragdon, President and Chief Executive Officer of Foundation for Government Accountability, the ACA’s expansion of Medicaid to able-bodied adults raised taxes for Americans and inhibited access to health care for the “severely disabled.”
He said that allowing adults without disabilities to access Medicaid blocked disabled adults from accessing the same benefits.
“Meanwhile, as that [expansion] happened, 700,000 Americans with intellectual and physical disabilities are stuck on Medicaid, Home and Community waiting lists while Obamacare’s able-bodied adults are always at the front of the line,” he said.
“Obamacare’s Medicaid expansion has left a trail of fiscal destruction. It’s prioritized able-bodied adults over the truly needy, elderly and disabled, and then it rewards money-laundering by states. That’s costly and wrong,” he added.
A conservative public policy think tank that focuses heavily on combating the expansion of Medicaid, the Foundation for Government Accountability has been at the forefront of attacks on the ACA.
Brian Blase, President of conservative think tank Paragon Health Institute said that the ACA sparked an affordability crisis for American taxpayers.
“The Inflation Reduction Act set the Covid credits to expire after 2025, and they should end. Continuing them with exacerbated fraud, increased premiums and health care prices drive out alternative financing arrangements, remove the imperative to perform this failing program, and drive the country into deeper debt,” Blase said.
According to Politico, Blase and the Paragon Health Institute played a critical role in the formation of policies that were adopted into $1 trillion in Medicaid cuts in the GOP’s spending bill.
Wisconsin resident Shana Verstegen, an ACA Marketplace Enrollee and member of MomsRising, an organization that has advocated for women’s health care, said that the growing cost of ACA premiums put a strain on her family’s finances. She said her family hasn’t gone on a vacation in years and had to consider “scaling back” her children’s sports activities.
She said that attacks on the ACA harm American families.
“Families like mine in every state: blue states and everywhere in between, rely on the Affordable Care Act. This is about real families, real kids and real health,” she said.
Verstegen said her family even considered withdrawing from her existing health care plan, but deemed it “too big of a risk.”
“Right now, we’re leaning toward my husband leaving a small business that he loves so that we can have affordable health care,” she said.
First signed into law in 2010, the ACA has long been a target of conservative attacks. Republicans argue that the coverage plan allows for the federal government to exert too much power over the health care system.
During the shutdown, discourse on Obamacare has become a focal point for both parties, as Democrats advocate for the extension of ACA tax credits while Republicans argue that excess spending for the health care plan places a strain on the federal budget.
While Republicans critique the cost of extending Obamacare subsidies, House Democrats like Minority Leader Hakeem Jeffries argue that the GOP has no substantial plan to lower health care costs and find an affordable alternative to the ACA.
“Mike Johnson has claimed over the last several weeks that Republicans are the party of health care. That’s a joke,” Jeffries said in a Thursday press conference.
“For several weeks, we were told that Republicans had a health care plan and that Republicans had planned all along to address the ACA issue and the fact that these tax credits for working class Americans, middle class Americans and everyday Americans are about to expire and Republicans can’t be bothered,” he added.
On the Democratic side of the subcommittee, Senator Richard Blumenthal (D-Conn.) said that the hearing was a part of a broader effort by Republicans to roll back the protections of the Affordable Care Act and cut spending for health care.
Blumenthal said that GOP-led efforts to cut spending for the ACA are “abhorrent.”
“It is a broad, relentless, calculated campaign to appeal the law that underlies those tax credits and take away health care insurance from millions and millions of Americans who would come to rely on it,” Blumenthal said.
“Republicans are refusing to extend enhanced credits because they hate the ACA more than they care about pain,” he said.
Senators raise competing legislation to continue SNAP benefits as suspension looms
WASHINGTON — In an attempt to curb a national humanitarian crisis when SNAP benefits — the Supplemental Nutrition Assistance Program that feeds nearly one in eight Americans — are set to be suspended nationwide on Nov. 1 due to the government shutdown, Democrats and Republicans are proposing separate bills to continue funding the program.
Sparring over who is to blame for the defunding, most Republicans maintain that Democrats must support Congress passing a clean bill to reopen the government. Meanwhile, Democrats have pushed back, insisting that the United States Department of Agriculture has already allocated contingency funds to support the benefits in the event of a shutdown.
“What brings us here today in an absolutely unbelievable way, President Trump is refusing to release the $5 billion in emergency funding for SNAP that helps feed 16 million kids, and that is a direct violation of the law,” Sen. Bernie Sanders (I-Vt.) said Wednesday afternoon.
The two parties have proposed two competing bills to continue SNAP benefits. On Tuesday, Sen. Ben Ray Luján (D-N.M.) introduced a bill that continues funding for SNAP and WIC, a nutrition program for Women, Infants and Children, supported by Democrats and by 11 Republicans. Sen. Josh Hawley (R-Mo.) put forward a similar bill on Oct. 21, co-sponsored by ten other Republicans and one Democratic senator, focused solely on SNAP funding.
Hawley’s effort was initially met with criticism by Senate Majority Leader Jon Thune (R-S.D.), with Republicans divided on the path forward.
“Even as nutrition programs are running out of money and federal workers are lining up with food banks, Democrats continue to reject every opportunity to end the shutdown or mitigate its pain,” Sen. Thune said.
Senate Minority Leader Chuck Schumer (D-N.Y.) responded by directly challenging Thune’s framing on the floor.
“The USDA said weeks ago that contingency funds were available to fund participant benefits,” Sen. Schumer said. “But now they’ve reversed course and literally wiped their plan from their own website. Because Donald Trump has ordered them not to use this funding.”
Over two dozen democratic attorneys general and governors are pursuing a lawsuit against the USDA for withholding these contingency funds. During the last government shutdown under the Trump Administration, SNAP benefits were maintained without pauses.
Experts say stress from uncertainty has already hit American households dependent on food assistance.
In the District of Columbia alone, 1 in 5 residents are on SNAP benefits. More than 54% of SNAP participants are in families with children and another 34% are in families with older adults or disabled members.
Kate Bauer, associate professor of nutritional sciences at the University of Michigan, works with families who rely on SNAP. She said misinformation around the program’s benefits fuels politicians to use public opinion to limit food assistance programs.
“There’s a belief that people on SNAP don’t work,” Bauer said. “There’s a belief that it goes to people who are here illegally. Those things are not true.”
SNAP lifted an average of 19,000 Washington D.C. residents above the poverty line annually between 2015 and 2019, including 8,000 children per year, according to the Center on Budget and Policy Priorities.
A mother on SNAP/EBT benefits from Washington, D.C., who did not want to be identified, said her future is ‘messed up’ while deliberations on continuing SNAP take place at the Capitol.
“I can’t feed my kids, and I can’t feed myself,” she said. “We’ve been heading up to Dollar Tree to get whatever we can get. It’s not fair.”
Lawmakers, experts warn U.S. could lose biotech edge to China
WASHINGTON — At a Senate Health, Education, Labor and Pensions committee hearing on biotechnology and U.S. competitiveness, lawmakers and witnesses warned that America risks losing its industry dominance.
China now accounts for 30% of global clinical trial starts, nearly matching the U.S. share of 35% and has expanded its global drug development pipeline eightfold, said John F. Crowley, president and CEO of the Biotechnology Innovation Organization.
Witnesses also highlighted systemic barriers to U.S. innovation, including outdated Food and Drug Administration (FDA) regulations, cuts to National Institutes of Health (NIH) funding, FDA layoffs and the increasing offshoring of early-stage clinical research.
“When developers are looking outside of the country for early-stage clinical work — we need to pick up our game,” Committee Chairman Sen. Bill Cassidy (R-La.) said in his opening statement.
Lowell Schiller, a scholar at the University of Southern California and a former FDA and Senate HELP committee staffer, advocated for streamlining FDA regulations to make the drug approval process more efficient.
Schiller gave the example of rare disease treatment developments, where traditional drug trials that involve randomized patients aren’t always possible due to small patient populations. In those cases, he suggests, the FDA could use alternative approaches such as relying on historic or real-world data.
Both Schiller and Crowley told the committee that offshoring parts of drug development — from early-phase clinical trials to manufacturing — is weakening U.S. leadership in the industry.
Crowley advocated for more investment in biotech startups, whereas Schiller said the FDA can make operating in the U.S. more globally competitive by adapting manufacturing regulations to current technology.
“With reforms like these, we can ensure that our country’s mature regulatory system continues to instill confidence in novel products and remains a competitive advantage for the United States,” Schiller said.
But Dr. Reshma Ramachandran, assistant professor of medicine at Yale University, sounded a warning about the impact of staffing cuts on the FDA’s ability to function effectively.
In early April, approximately 3,500 employees were laid off at the FDA as part of a larger workforce reduction in the Department of Health and Human Services by the Trump administration.
“The recent firing and attrition of more than 20% of the FDA workforce, including over 900 scientists and technical experts … threatens the U.S.’s ability to continue critical regulatory operations and implement solutions that deliver a sustainable supply of treatments that work,” Ramachandran said.
Beyond regulatory reforms, witnesses emphasized the importance of federal research funding to NIH and academic institutions. Dr. Aaron Kesselheim, a Harvard Medical School professor, noted that all 42% of recent new biological drugs had late-stage reliance on public funding. He also added that all FDA-approved gene therapies can be traced back to federally supported academic institutions or their spinoffs.
But the health budget for 2026 includes a 40% cut to NIH. Kesselheim urged the Congress to revert to the previous level of research funding.
“Congress must reestablish the normal flow of research funding before the U.S. scientific establishment in a new generation of innovative biotechnology treatments is irreparably damaged,” Kesselheim said.
Sen. Patty Murray (D-Wash.) reinforced this concern, noting that the Trump administration terminated $2.3 billion in NIH funding and canceled roughly 500 grants.
Turning the focus back to global dominance, Sen. Andy Kim (D-N.J.) said the committee and the nation must embrace the urgency of the competition it faces from China. Kim added that the innovative use of artificial intelligence could be key to accelerating drug research.
Crowley underscored that while the U.S. is currently a global leader in biotechnology, the tide may shift in two to three years.
“We need to act boldly and we need to act today,” Crowley. “We believe in two to three years, we can lose this.”
Financial pressures mount for rural hospitals as Federal support programs expire
WASHINGTON — Health care administrators across rural America say financial pressures are mounting as federal support programs expire and Medicaid cuts take effect, putting many facilities at risk of closure.
In Hugo, Colorado — a town of fewer than 1,000 people — that reality is familiar. Lincoln Health, a 25-bed hospital and the only facility on the nearly 600-mile stretch of I-70 between Denver and Kansas City, Missouri, has faced financial strain for years.
“If you drive east on I-70, you care about my hospital because I’m the only thing out here if something should happen,” said Kevin Stansbury, Lincoln Health’s CEO. “We do a lot, and we do it not because any of those things are terribly lucrative. We do it because there’s no one else out here to do those things.”
Last month, Lincoln Health closed its assisted living facility due to financial constraints. Stansbury said the hospital is still evaluating how to maintain its remaining services as Medicaid cuts hit and key federal programs expire.
The federal reconciliation bill, signed into law on July 4, is projected to cut federal Medicaid spending by $911 billion over the next decade and increase the number of uninsured Americans by 10 million, according to the Congressional Budget Office. The reductions are set to take effect over the next two years.
In rural areas, federal Medicaid spending is projected to decline by $137 billion over the next decade, according to estimates from the Kaiser Family Foundation. Roughly three-quarters of Lincoln Health’s patients are covered by Medicaid or Medicare, and even before the cuts, reimbursement rates were low, Stansbury said.
Several federal programs that offered financial support to rural hospitals lapsed on September 30, including the Medicare-Dependent Hospital program, which provided enhanced payments to hospitals with a high proportion of Medicare patients, and the Low-Volume Adjustment program, which offered additional payments to hospitals with low annual discharges.
The Medicaid Disproportionate Share Hospital program, which offsets uncompensated care costs for hospitals serving a high number of Medicaid and uninsured patients, saw $8 billion in cuts on October 1.
“Not knowing whether those payment adjustments will continue is incredibly difficult for hospital administrators to be able to plan long term because they don’t know whether or not they will continue receiving those payments,” Alexa McKinley Abel, director of government affairs & policy at the National Rural Health Association, said.
Abel added that many hospitals have already been budgeting under the assumption that the cuts will remain in place.
Roughly half of the nation’s rural hospitals currently operate at a loss, according to the National Rural Health Association. Stansbury described challenges that Lincoln Health shares with many rural hospitals, including low commercial reimbursement rates and limited access to capital.
A study by the Colorado Rural Health Center found that rural eastern hospitals receive commercial payments averaging 139% of Medicare rates, compared with 240% in Denver.
“They’re just going to try to drive me as low as they possibly can,” Stansbury said. “And what it seems to be forgetting is that if I go out of business, then there’s a big area of the state that doesn’t have health care.”Moreover, built in 1959, Lincoln Health has had limited resources for major renovations. Operating on tight margins leaves little room for upgrades or construction, he said.
In some rural areas, maternity care is estimated to be the first to shut down due to its high operating costs, according to Denae Herbert of the Louisiana Rural Health Association.
“There’s not sufficient volume to really sustain a birthing center,” Herbert said. “So if there is a rural hospital still providing that service, that would certainly be at risk as well, which is very concerning, particularly because of the maternal mortality rate in Louisiana being as high as it is, we need to increase access to maternal health care, not decrease it.”
According to a 2024 report by the Center for Healthcare Quality and Payment Reform, 75% of rural hospitals in Louisiana don’t offer maternal care. The state’s maternal mortality rate stands at 37.3 deaths per 100,000 live births — among the highest in the country.
A June letter from Senate Democrats estimated that 33 rural hospitals in Louisiana are at risk of closing following the cuts.
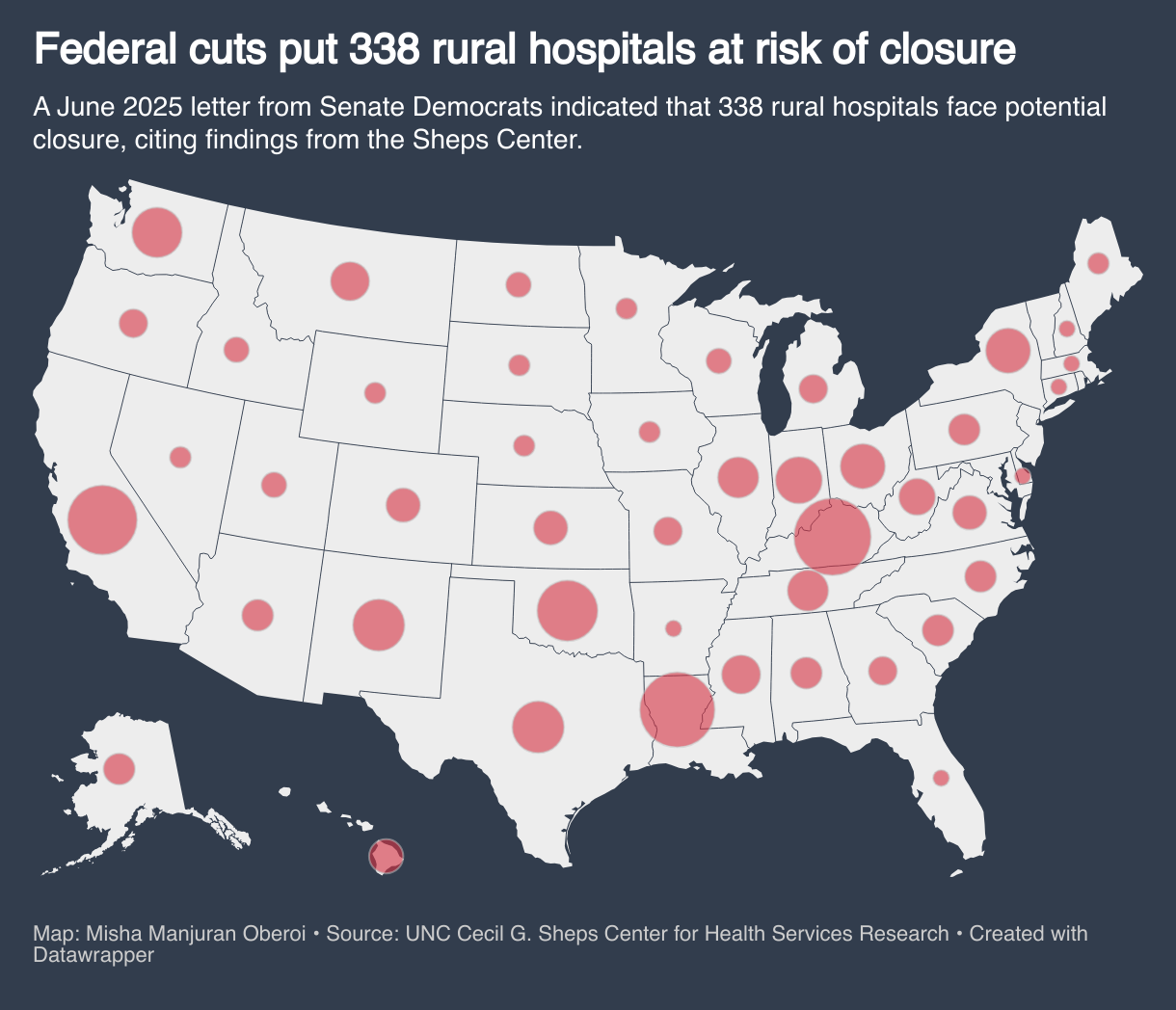
In Virginia, that number amounts to six. But according to Sen. Mark Warner (D-Va.), these hospitals are concentrated in areas that voted overwhelmingly for President Donald Trump.
“The irony of this is that these were the communities that frankly — they voted for Trump because they wanted to lower costs,” Warner said. “Well, we’ve not seen groceries go down, we’ve not seen inflation go down, and states are seeing health care costs skyrocket.”
Lee County Community Hospital, one of the six at risk of closing under the cuts, is part of a county that voted 85.7% for Trump, according to Politico’s election map.
The situation in Oregon is similar, according to Sen. Ron Wyden (D-Ore.). He said he recently led a series of town hall meetings in rural Oregon, in communities that voted 70% for Trump. He said people are aware that a “health care wrecking ball is coming right at them.”
Wyden also echoed Herbert’s concerns about the potential increase in maternity deserts nationwide.
“You can’t have rural life without rural health care, but we are headed in that direction,” Wyden said.
While inpatient rural hospital care is facing setbacks, so is virtual care. The telehealth waiver enacted during the COVID-19 pandemic expired on Oct. 1. In most cases, providers will no longer be reimbursed for telehealth visits delivered to Medicare patients in their homes.
Abel said this is a major concern because telehealth has the potential to improve rural health care significantly. She said a longer extension of the flexibilities would have been beneficial for rural areas.
“There’s been studies showing that uptake in rural areas for telehealth has actually been less compared to in urban areas, and I think that’s because the infrastructure is not fully there yet, and without knowing that these flexibilities will be in place for the long term, it’s hard for providers to invest in it,” Abel said.
Stansbury says that while telehealth is an additional challenge, it is not a substitute for in-person care.
“If somebody gets in an automobile accident on I-70, telemedicine does nothing for that,” he said. “I need people on the ground who are able to receive those patients and take care of them effectively.”
For patients who rely on these hospitals daily, the combination of aging facilities and policy changes is tangible. Limon, Colorado resident Lorie Coonts has been using Lincoln Health’s services for four decades. Despite the hospital’s deteriorating condition, including shared bathrooms and the absence of OB-GYN services, Coonts said the hospital is like “family taking care of family.”
She said she worries about the hospital’s financial instability and risk of closure, noting that if Lincoln Health were to close, the small community would dwindle further.
“It just feels like the hospitals are faced with one thing and one after the other,” Coonts said. “It just feels like it’s more and more mandates and rules … that just keep things from being easy and being able to afford it. Every time we turn around we get slapped in the face with something else.”
Published in conjunction with 
Senate weighs AI’s role in health care amid safety, regulation concerns
WASHINGTON – At an Oct. 8 Senate Health, Education, Labor and Pensions Committee (HELP) hearing, lawmakers examined how artificial intelligence is reshaping health care — from easing paperwork to raising new safety concerns, including reports of chatbot-linked teen suicides.
Sen. Bill Cassidy (R-La.), chairman of the committee, set the tone of the hearing during his opening statement, highlighting AI’s potential to accelerate drug discovery and lower health care costs while warning of its darker consequences, including recent parent allegations that chatbots induced teen suicides.
“There is enormous potential to improve people’s lives; there is enormous risk,” Cassidy said.
Stanford bioengineering professor Dr. Russ B. Altman, a witness at the hearing, said AI can change health care in three main ways: augmenting clinical diagnoses, giving providers more time with patients and giving patients more control over their care.
In response to Altman’s testimony, Sen. Susan Collins (R-Maine) broached the subject of whether AI can help struggling rural hospitals, which she said are “teetering on the brink of closure.”
Altman said AI is both an opportunity and a challenge for rural hospitals. He says it could potentially help hospitals provide more specialized care closer to home.
“I think that this is a great opportunity to extend the capabilities of rural hospitals but I think they would tell you right now that they need help in vetting these tools and right now it’s a tsunami that they can’t manage,” Altman said.
He proposed creating an oversight body that lays out best practices, vets tools and formulates guidelines for hospitals, as a solution.
A recurring topic at the hearing was the recent examples of chatbot-associated teen suicides — most notably, at a judiciary hearing last month, Florida mother Megan Garcia alleged that prolonged abuse by AI chatbots on a platform called Character.AI led to her 14-year-old son’s suicide.
Sen. Josh Hawley (R-Mo.) posed the question of how AI can be regulated to prevent the “killing of kids” to witness John Bailey, a senior fellow at the American Enterprise Institute.
“Aren’t we beyond there being a potential problem that maybe we need to have a little further development before they release the models?” Hawley asked. “Doesn’t Congress need to do something now in order to protect kids from being killed by AI systems?”
Bailey said researchers don’t fully understand why chatbots behave in harmful ways and called for human intervention when conversations become dangerous, as well as greater transparency from companies.
Hawley pushed back, stating that he’s beyond the point of transparency and wants companies to “stop killing kids.”
Several lawmakers returned to the issue throughout the hearing, including Sen. Jon Husted (R-Ohio) who directed the committee to a bill he recently introduced: Children Harmed by AI Technology Act of 2025 (CHAT).
The bill requires owners and operators of AI companion chatbots to bar minors from accessing adult content and parental consent for minors to use chatbots. It would also mandate the chatbot immediately inform consenting parents if the conversation with a child includes self-harm or suicidal ideation.
Sen. Ashley Moody (R-Fla.) said that companies should be held liable for their chatbots causing harm or death to users. She also posed the question of how lawmakers can regulate AI.
Both Altman and Bailey said any regulation should begin with clearly defining who is responsible when AI systems cause harm.
“I think we need principles of where does liability fall there as it relates to the developers of AI, the deployers of AI and then how does that relate to both users and then also AI agents,” Bailey said.

Medill Today | Tuesday, March 10, 2026